
Relative energy deficiency in
Just to stay alive while lying in bed all day requires energy from food intake. This caloric number is roughly equivalent to your resting metabolic rate. Exercise (training) requires additional energy from food intake — the energy from everything you eat is partitioned by your body to cover these two demands. When we subtract the energy needed to cover the demands of exercise training from the energy consumed, the residual energy is known as energy availability (EA) and is expressed as kcal/kg of lean body mass.
The exact EA value to maintain health will vary between individuals depending on their body composition and age, but if EA falls below the minimal level required for an individual, the body goes into a state of low energy availability (LEA) or essentially energy-saving mode. Imagine a mobile phone with a low battery, which will switch off non-essential apps to save energy.
For females in LEA, the obvious clinical warning sign is the disruption and cessation of menstruation. This is probably why LEA was first described as part of the female athlete triad, which is comprised of disordered eating, menstrual disruption, and deterioration of bone health. The female athlete triad excludes half the population (men), and the consequences of LEA are not limited to menstruation and the skeletal system. This is why RED-S is a better clinical model, which includes male exercisers.
How Does Low Energy Availability Occur?
The diagram shows how you can end up in a state of LEA, whether unintentionally or intentionally. The central column shows an athlete who is taking in enough nutrition to cover energy demands from training, with enough energy remaining to cover requirements for life processes. In the bar on the left, the athlete has reduced energy intake, but energy demand from training has remained the same, resulting in LEA. Conversely, in the bar on the right, although the athlete has maintained the same energy intake, the training load has increased — resulting in LEA.
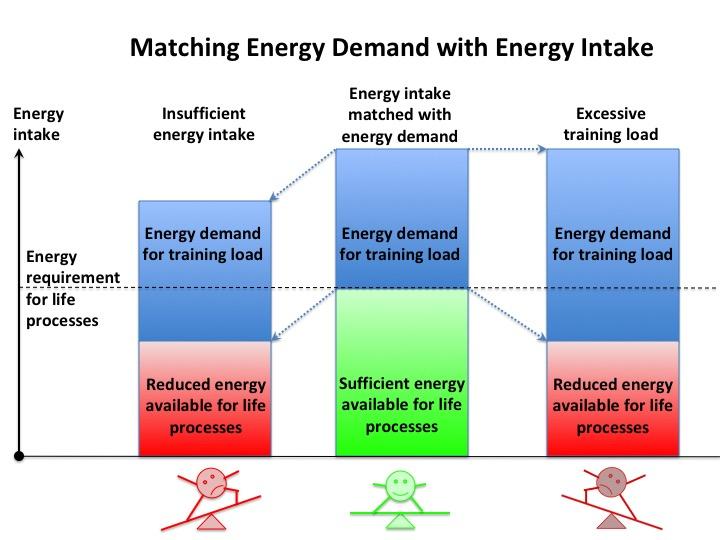
Reproduced with permission Dr. N. Keay BJSM and BASEM
What are the Symptoms of RED-S?
RED-S results in adverse health and athletic performance consequences. As mentioned above, when in LEA, the body will try to save energy by putting some systems into “energy saving mode,” including the slowing of bone turnover. This increases the risk of bone stress responses, including stress fracture. The body will also dampen the production of hormones in the reproductive system, including oestrogen and progesterone in women and testosterone in men. Hormones are important for driving the adaptations to exercise, so any disruption of this system, including that caused by LEA, will reduce the effectiveness of training and, hence, athletic performance.
Be aware even short-duration energy deficits, for example, those that can occur during a long bike ride, have been shown to disrupt hormones in both males and females. Sustaining LEA long-term quite simply limits your ability to reach your full athletic potential.
LEA may manifest as a recurrent injury or illness and/or the inability to adapt to training stimuli to improve performance. This situation was found in a recent study of 50 competitive male cyclists, where those in chronic LEA had significantly worse bone health and lower 60-minute functional threshold power (FTP) for a given training load compared to those cyclists with adequate EA.
Who is at Risk of Developing RED-S?
Athletes at risk of developing RED-S are those involved in gravitational sports where a high power-to-weight ratio confers a performance advantage (i.e., road cyclists, runners, triathletes and climbers), weight category sports such as boxing and lightweight rowing, and aesthetic sports including diving, gymnastics, and dance.
RED-S can occur in any age or level of athlete. Young athletes or dancers are at particular risk of developing RED-S, as puberty is already a high-energy demand state. LEA can have rapid onset when coupled with training demands and/or emphasis on low body weight for sport or dance and can compromise growth and development. Nevertheless, injury issues (including stress fractures) may not occur until moving from junior to senior or professional ranks, when the training load increases.
How to identify RED-S?
In the situation of sustained LEA, the metabolic rate will slow to conserve calories, and the hormonal changes will signal the body to increase body fat and decrease muscle. Therefore, it becomes increasingly difficult to lose weight or change body composition in LEA, which the athlete may interpret as not restricting enough or training hard enough. In other words, it’s very easy for a vicious circle to develop.
So if weight loss is not a sign of LEA, what is? In females of reproductive age, regardless of how much exercise is being undertaken, menstrual periods are a sign that hormones are at a healthy level. Regular menstruation could even be considered a training metric, as shown by Gwen Jorgensen in her TrainingPeaks plan, which she made public last year. Other indicators suggestive of LEA in both male and female athletes are:
- Recurrent injury (soft tissue and/or bone)
- Recurrent Illness
- Unexpected fatigue
- Disrupted sleep patterns
- Change in mood
- Reduced social interaction
- Problematic relationship with food and/or training
- Stagnation and deterioration in performance
What to do about RED-S?
Being alert to athletes at risk of RED-S is vital — this is where coaches and mentors play a crucial role. In the first instance, excluding underlying medical conditions is important. The signs and symptoms suggestive of RED-S are not exclusive to LEA, so checking some baseline markers to rule out things like infection, specific nutritional deficiencies, or endocrine conditions is advisable.
Once medical conditions have been ruled out and diagnosis of RED-S established, the good news is that there are three key factors under an athlete’s control, which can improve EA and, therefore, optimize health and performance. These factors are training load, nutrition, and recovery. Integrating periodization of these key factors will need careful guidance from a coach and, ideally, a medic and clinical dietician.

A word of warning for female athletes: there is evidence to show that taking an oral contraceptive pill (OCP or any hormonal type of contraception) will not protect bone health. In fact, recent research shows that this could make bones worse. An OCP produces withdrawal bleeds due to synthetic, external hormones — not menstrual periods due to your own, internally-made hormones. Although being on an OCP may be reassuring, it masks what is really going on with hormones.
Where to go from here?
References
IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update Mountjoy M, Sundgot-Borgen J, Burke et al British Journal of Sports Medicine (2018) 52(11) 687-697 DOI: 10.1136/bjsports-2018-099193
Raising Awareness of RED-S in Male and Female Athletes and Dancers BJSM
Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists Keay N, Francis G, Hind K BMJ Open Sport and Exercise Medicine (2018) 4(1) DOI: 10.1136/bmjsem-2018-000424
How do you identify male cyclist at risk of RED-S? BJSM
The modifiable factors affecting bone mineral accumulation in girls: The paradoxical effect of exercise on bone Keay N Nutrition Bulletin DOI: 10.1046/j.1467-3010.2000.00051.x
2018 UPDATE: Relative Energy Deficiency in Sport (RED-S) BJSM
BASEM Health4Performance educational website
London NHS RED-S Clinic, Royal National Orthopaedic Hospital (RNOH)





